Eosinophilic Myocarditis Due To Eosinophilic Granulomatosis With Polyangiitis (Churg-Strauss sydrome)
A 66-years-old patient with a history of bronchial asthma, recurrent respiratory infections and episodes of rhinitis presented with progressively worsening dyspnea (NYHA III). Laboratory findings revealed elevated hsTnT levels, hypereosinophilia on CBC and cutaneous purpura on lower extremites.

ECG demonstrated nonspecific negative T-wave inversions in leads I, II, aVL, aVF, pathological Q waves in V1-V2 and ST-segment depresions in V4-V6.

Bedside echocardiography revealed mildly reduced systolic function (EF 40-45%) with diffuse hypokinesis predominantly affecting the anterior wall and pericardial effusion (max. 12 mm).

INITIAL ASSESSMENT
Clinical examination:
• heart rate 96 bpm, blood pressure 129/85 mmHg, temperature 36.4°C
• oxygen saturation 95% on room air
• basal attenuation of breath sounds with bilateral crackles
• no peripheral edema
Laboratory results:
Liver biochemistry showed mild enzyme elevation, including alkaline phosphatase 4.3 µkat/L (reference 0.58–1.75µkat/L), AST 1.00 µkat/L (0.17–0.75 µkat/L), and GGT 4.75 µkat/L (0.20–1.07µkat/L), with normal total bilirubin 4.0 µmol/L (3.4–20.0 µmol/L).
Inflammatory markers were elevated, with CRP 104 mg/L (reference 0–5 mg/L), while procalcitonin remained low at 0.10 µg/L (0–0.5 µg/L).
Cardiac biomarkers were elevated, with high-sensitivity troponin T 1674 ng/L (0–16 ng/L) and NT-proBNP 7569 ng/L (0,0–125 ng/L).
Complete blood count demonstrated leukocytosis 18.5 ×10⁹/L (4–10 ×10⁹/L), marked hypereosinophilia 12.8 ×10⁹/L (0-0.5 ×10⁹/L), normal hemoglobin 124 g/L (120–160 g/L), and normal platelet count 373 ×10⁹/L (150–400 ×10⁹/L).
Immunological testing revealed positive rheumatoid factor 141 kIU/l (reference 0-30), Eosinophil cationic protein (ECP)>200 µg/L (0-15µg/L), total IgE 4639 kIU/L (2-150 k IU/L) and IgG4 7.39 g/L (0.04-0.86 g/L). ANA, ENA, dsDNA, ANCA, MPO, PR3 antibodies were negative.
Coronary angiography was performed with normal finding.
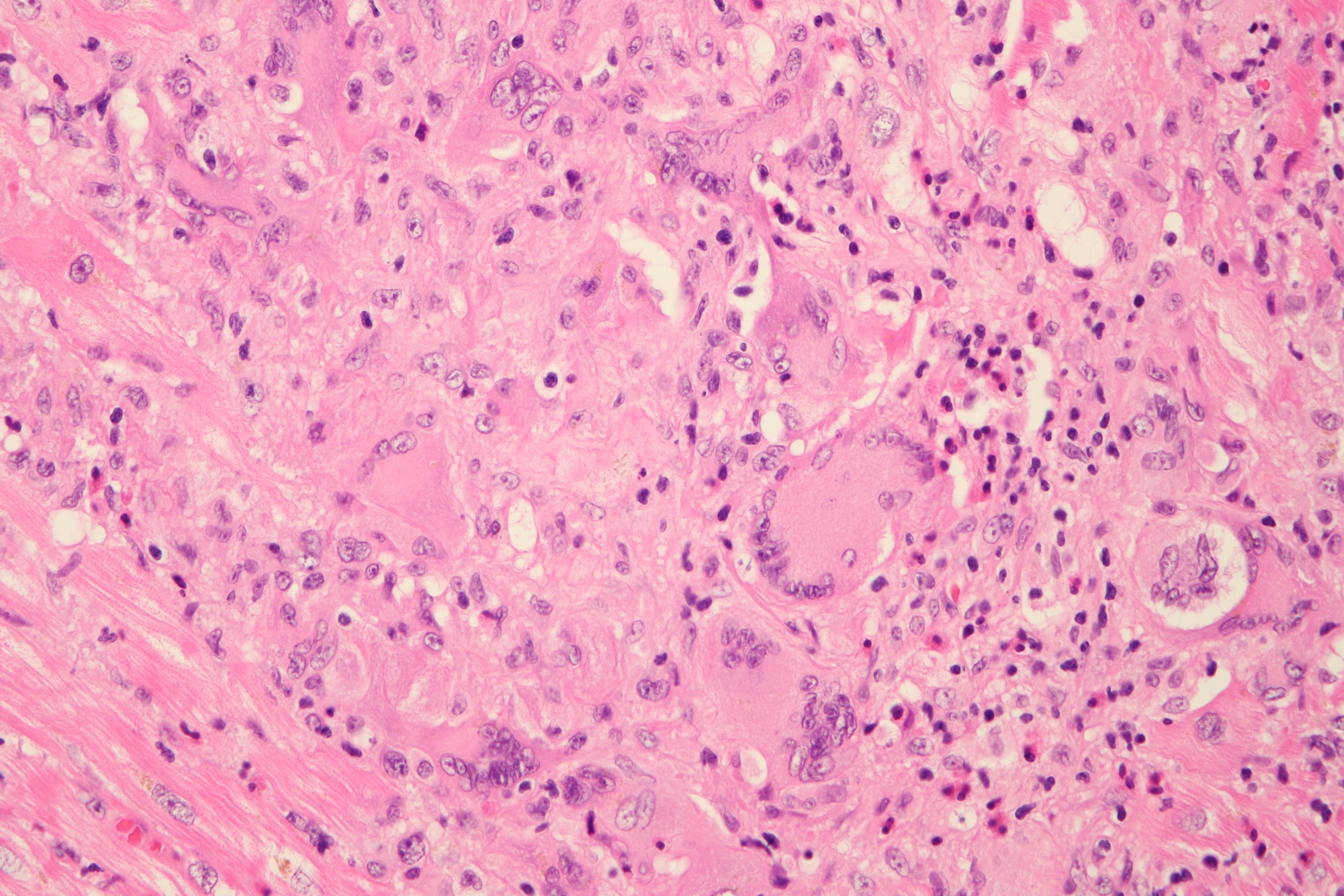
Subsequently Endomyocardial biopsy was iperformed with following findings:
• mild fibrosis with disperse eosinophilic inflammatory infiltrate (arrow on an image)
• small focus of cardiomyocyte necrosis associated with forming an eosinophilic"microabscess"
• no granulomas or multinucleated giant cells
• staining for amyloid (Congo red) and iron is negative
• no morphological evidence of fungal (PAS stain), viral, or parasitic infection

Cardiac MR revealed:
• dilated left ventricle (EDVi 125 ml/m2), left ventricular ejection fraction 38%
• diffuse hypokinesis, subendocardial LGE in apex
• mild mitral regurgitation (regurgitant fraction 8%)
• small circumferential pericardial effusion, mild bilateral pleural effusions
Cutaneous biopsy from cutaneous purpura was also performed: mild superficial perivascular dermatitis with occasional eosinophils within the inflammatory infiltrate
Chest CT showed no evidence of interstitial lung disease, only small areas of ground-glass opacity consistent with peribronchiolitis along with small pleural effusions and mediastinal lymphadenopathy.
MANAGEMENT:
Abovementioned findings were consistent with a suspected diagnosis of eosinophilic myocarditis. In the differential diagnosis, a drug-induced hypersensitivity reaction and hypereosinophilic syndrome (HES) remain under consideration. Hematological evaluation, laboratory genetic testing, and assessment for thrombophilic states are being performed to exclude HES.
The patient was treated with intravenous methylprednisolone 1 g daily for three consecutive days, resulting in a good clinical and laboratory response. Subsequently, oral prednisone 20 mg (2-1-0) was initiated in combination with rituximab (1000 mg initially and 1000 mg after 2 weeks). Prophylaxis against Pneumocystis jirovecii pneumonia was started - cotrimoxazole 400/80 mg. Anticoagulation with enoxaparin 0,6 ml s. c. 1-0-1 and heart failure treatment with empagliflozin 10mg, losartan 50mg and metoprolol 25 mg were initiated.
Echocardiography on 10th day of hospitalization:• mildly dilated left ventricle (LVEDD 59mm, LVESD 29 mm)
• preserved left ventricular ejection fraction (55–60%)
• mild mitral regurgitation (1-2/4), mild tricuspid regurgitation (2/4)
• pericardial effusion (max. 12 mm) in A4C
After clinical improvement, the patient was then transferred to the Institute of Rheumatology for further management and follow-up treatment.
DISCUSSION:
Eosinophilic granulomatosis with polyangiitis (Churg–Strauss syndrome) is a rare, chronic, multisystem inflammatory disease characterized by asthma, rhinitis, nasal polyps, peripheral blood eosinophilia,and tissue eosinophilia on biopsy. EGPA may affect multiple organ systems, including the cardiovascular, gastrointestinal, renal, cutaneous, and central nervous systems.
Cardiac involvement is one of the most serious manifestations of EGPA and represents a major cause of mortality. Cardiac manifestations include heart failure, eosinophilic myocarditis, endocarditis, pericarditis, cardiomyopathy, valvular disease (regurgitation orstenosis), coronary artery disease, and cardiac rhythm abnormalities. Patients with cardiac involvement are less likely to be ANCA-positive and tend to have higher peripheral eosinophil counts than other patients with EGPA.
Diagnosis
The diagnosis of EGPA is based on acombination of marked eosinophilia (≥1000 cells/μL), characteristic clinical features (e.g., asthma, chronic rhinosinusitis with or without nasal polyposis,mononeuritis multiplex), and histopathological findings demonstrating eosinophilic inflammation and/or small- to medium-vessel vasculitis in affected tissues. The following classification criteria may support the diagnosis; however, they are not intended for diagnostics.
2022 ACR/EULAR Classification Criteria for EGPA (A score of ≥6 points has a sensitivity of 85% and a specificity of 99% for the classification of EGPA.)
· Blood eosinophil count ≥1000cells/μL (+5 points)
· Asthma (+3 points)
· Nasal polyps (+3 points)
· Extravascular eosinophil-predominant inflammation on biopsy (+2 points)
· Mononeuritis multiplex or motorneuropathy not due to radiculopathy (+1 point)
· Hematuria (−1 point)
· Positive cytoplasmic ANCA (cANCA) or anti-proteinase 3 (PR3) antibodies (−3 points)
Prognosis
Survival has improved significantly to approximately 70–90% at 5 years with modern therapy. The leading causes of death remain cardiac failure, myocardial infarction, and gastrointestinal bleeding.
The Five-Factor Score (FFS) is used to predict mortality risk in patients with established EGPA. The score includes five adverse prognostic factors associated with reduced survival:
· Cardiac insufficency
· Absence of ENT manifestations
· Renal insufficiency (serum creatinine >150 μmol/L)
· Age >65 years
· Gastrointestinal involvement
Treatment
Patients with organ- or life-threatening manifestations, particularly those identified by the Five-Factor Score, should receive high-dose glucocorticoids as initial therapy, followed by cyclophosphamide or rituximab or combination therapy regimen for remission induction. Early initiation of anti–IL-5 therapy, such as mepolizumab or benralizumab, may reduce eosinophilic inflammation, decrease glucocorticoid therapy, and help maintain disease remission. For patients with non-severe EGPA, who are refractory to glucocorticoid monotherapy, alternative induction regimens include glucocorticoids combined with methotrexate or mycophenolate mofetil,which may provide effective disease control with lower treatment-related toxicity.
Remission Maintenance
Remission is characterized by an absence of any clinical manifestation arising from ongoing vasculitis and is usually achieved within 6–12 weeks. Patients are transitioned to a maintenance regimen to prevent disease relapse. Anti-IL-5/5R therapies are preferred for maintenance due to their efficacy and lower toxicity profile compared to traditional immunosuppressants. Glucocorticoids are gradually tapered over 3 to 18 months to the lowest effective dose. Approximately 40% of patients on maintenance anti-IL-5 therapy can fully discontinue glucocorticoids within a year. Maintenance therapy is typically continued for at least 12 to 18 months, though indefinite therapy may be necessary for those with multiple relapses.
The Birmingham Vasculitis Activity Score (BVAS) is a standard tool for quantifying disease activity.
Relapses are common, especially during steroid tapering. Severe relapses require re-induction, while non severe relapses often managed by increasing the glucocorticoid dose back to the last effective level followed by a slower taper.
REFERENCES:
1. Paneez Khoury, MD, MHSc,Clinical features and diagnosis of eosinophilic granulomatosis withpolyangiitis (EGPA), Treatment and prognosis, Uptodate database.
2. Solans-Laqué R, Rúa-Figueroa I,Blanco Aparicio M., Red flags for clinical suspicion of eosinophilicgranulomatosis with polyangiitis (EGPA), European Journal of Internal Medicine,2024; 128, 45-52.
3. Srikantharajah M, Gopalan D,Wilson-Morkeh H, Siddiqui S, McAdoo SP, Youngstein T. Cardiac Involvement inEosinophilic Granulomatosis with Polyangiitis. Curr Cardiol Rep. 2025 Jul9;27(1):109. doi: 10.1007/s11886-025-02258-z. PMID: 40632386; PMCID:PMC12241301.
4. Adi Miller-Barmak, YonatanButbul Aviel, Mepolizumab treatment for eosinophilic granulomatosis withpolyangiitis (EGPA) with cardiac involvement, Rheumatology, Volume 64, Issue11, November 2025, Pages 5993–5994,
AUTHORS:
Simona Loziňáková, Michal Pazdernik, Ondřej Fabián
.jpg)
You Might Also Like
Eosinophilic Myocarditis Due To Eosinophilic Granulomatosis With Polyangiitis (Churg-Strauss sydrome)
Cardiogenic shock due to Giant Cell Myocarditis