
Introduction
- premature ventricular complexes (PVCs) might be present among patients with heart disease, but also in healthy population including in children, although the prevalence of PVCs increases with age and a history of heart disease
- mechanisms of PVCs generally include triggered activity, automaticity and reentry or their combination
- PVCs may be symptomatic or asymptomatic and found incidentally
- symptomatic patients may present with palpitations, chest discomfort, presyncope, fatigue or dyspnea
- PVCs can trigger different type of arrhythmia especially when the R on T phenomenon occurs
- the diagnosis can be made by documenting a PVC on a 12lead ECG (which can determine the probable origin of the PVC), but longer term recordings such as 24hour Holter monitoring are more likely to capture PVCs if they are less frequent and give the possibility to assess the PVC burden (PVCs as a percentage of all the beats) which is used in the decision making process for an appropriate treatment
Classification
- Triplet - three consecutive PVCs, however, three or more consecutive PVCs lasting up to 30 s are usually described as non sustained ventricular tachycardia
ECG characteristics
- the QRS complex occurs earlier than expected = premature
- the QRS complex is abnormal in shape and duration usually exceeds 120ms (exceptions apply as the duration depends on origin of the PVC, examples of a narrow complex PVCs are fascicular to inter ventricular septal origin
- the morphology of the PVC (LBBB, RBBB) can be used to determine the origin of the PVC
- the QRS complex may either follow a P wave that is not conducted or it is not preceded by a P wave at al
- a PVC is followed by:
- a compensatory pause = the next QRS occurs at two times the preceding R-R interval
- a noncompensatory pause = the atria are retrogradely activated and the sinus node is reset, the next QRS occurs after an interval other than two times the preceding R-R interval
- no pause - an interpolated PVC is followed by a sinus beat with a slightly prolonged PR interval but without a pause
- a ventricular echo - the impulse initially propagates retrogradely but reverses its direction and returns to activate the ventricles after a delay
Management
- depends on symptoms, PVC burden and presence of heart disease
- asymptomatic PVCs in healthy patients do not warrant any treatment but the patient should be followed if the PVC burden is high
- for patients with symptomatic PVCs pharmacotherapy should be considered using beta blockers as a first line therapy
- other drugs (such as flecainide, amiodarone and others) may be considered but are used less often and many of them have considerable side effects and contraindications
- catheter ablation should be considered in patients with significant symptoms, high load of PVCs and in those with reduced ejection fraction
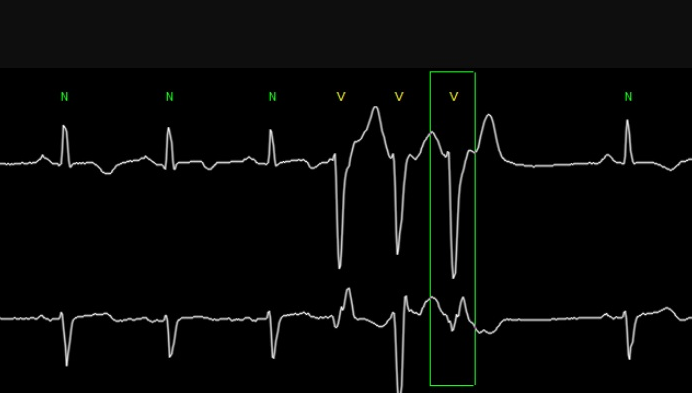
ECG 1 Triplet of PVCs
References
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 11th ed, Zipes DP, Libby P, Bonow RO, et al, W.B. Saunders Company, Philadelphia 2018.
- Marcus, Gregory M. 2020. “Evaluation And Management Of Premature Ventricular Complexes”. Circulation 141 (17): 1404-1418. https://doi.org/10.1161/CIRCULATIONAHA.119.042434.
- Silvia G Priori, Carina Blomström-Lundqvist, Andrea Mazzanti et al. ESC Scientific Document Group, 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC) Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), European Heart Journal, Volume 36, Issue 41, 1 November 2015, Pages 2793–2867, https://doi.org/10.1093/eurheartj/ehv316
- https://litfl.com/premature-ventricular-complex-pvc-ecg-library/
Published by

Assoc. Prof. Michal Pazderník, MD, Ph.D. FESC
Introduction
- premature ventricular complexes (PVCs) might be present among patients with heart disease, but also in healthy population including in children, although the prevalence of PVCs increases with age and a history of heart disease
- mechanisms of PVCs generally include triggered activity, automaticity and reentry or their combination
- PVCs may be symptomatic or asymptomatic and found incidentally
- symptomatic patients may present with palpitations, chest discomfort, presyncope, fatigue or dyspnea
- PVCs can trigger different type of arrhythmia especially when the R on T phenomenon occurs
- the diagnosis can be made by documenting a PVC on a 12lead ECG (which can determine the probable origin of the PVC), but longer term recordings such as 24hour Holter monitoring are more likely to capture PVCs if they are less frequent and give the possibility to assess the PVC burden (PVCs as a percentage of all the beats) which is used in the decision making process for an appropriate treatment
Classification
- Triplet - three consecutive PVCs, however, three or more consecutive PVCs lasting up to 30 s are usually described as non sustained ventricular tachycardia
ECG characteristics
- the QRS complex occurs earlier than expected = premature
- the QRS complex is abnormal in shape and duration usually exceeds 120ms (exceptions apply as the duration depends on origin of the PVC, examples of a narrow complex PVCs are fascicular to inter ventricular septal origin
- the morphology of the PVC (LBBB, RBBB) can be used to determine the origin of the PVC
- the QRS complex may either follow a P wave that is not conducted or it is not preceded by a P wave at al
- a PVC is followed by:
- a compensatory pause = the next QRS occurs at two times the preceding R-R interval
- a noncompensatory pause = the atria are retrogradely activated and the sinus node is reset, the next QRS occurs after an interval other than two times the preceding R-R interval
- no pause - an interpolated PVC is followed by a sinus beat with a slightly prolonged PR interval but without a pause
- a ventricular echo - the impulse initially propagates retrogradely but reverses its direction and returns to activate the ventricles after a delay
Management
- depends on symptoms, PVC burden and presence of heart disease
- asymptomatic PVCs in healthy patients do not warrant any treatment but the patient should be followed if the PVC burden is high
- for patients with symptomatic PVCs pharmacotherapy should be considered using beta blockers as a first line therapy
- other drugs (such as flecainide, amiodarone and others) may be considered but are used less often and many of them have considerable side effects and contraindications
- catheter ablation should be considered in patients with significant symptoms, high load of PVCs and in those with reduced ejection fraction
ECG 1 Triplet of PVCs
References
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 11th ed, Zipes DP, Libby P, Bonow RO, et al, W.B. Saunders Company, Philadelphia 2018.
- Marcus, Gregory M. 2020. “Evaluation And Management Of Premature Ventricular Complexes”. Circulation 141 (17): 1404-1418. https://doi.org/10.1161/CIRCULATIONAHA.119.042434.
- Silvia G Priori, Carina Blomström-Lundqvist, Andrea Mazzanti et al. ESC Scientific Document Group, 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC) Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), European Heart Journal, Volume 36, Issue 41, 1 November 2015, Pages 2793–2867, https://doi.org/10.1093/eurheartj/ehv316
- https://litfl.com/premature-ventricular-complex-pvc-ecg-library/
Published by
Assoc. Prof. Michal Pazderník, MD, Ph.D. FESC




