
Introduction
- Bifascicular block is a combination of a right bundle branch block (RBBB) and a block of one of the left bundle branch fascicles – left anterior fascicular block (LAFB) or left posterior fascicular hemiblock (LPFB)
- This means that 2 of the 3 main conducting pathways through the ventricles are blocked
- Bifascicular block occurs in approx. 1% to 2% of the adult population
Causes
- Bifascicular block is often associated with structural heart disease and may be associated with progression to high-grade block or complete heart block
- The rate of progression to complete AV block is 1% to 4% per year
- In patients with syncope the rate goes up to 17% and is also associated with the presence of malignant ventricular arrhythmias
- Block in either the LAF or LPF of the LBB produces axis deviation - the overall direction of the QRS complex is shifted toward the site of the block
RBBB + Left anterior fascicular block
- more common than RBBB + LPH
- RBB and LAF have a single coronary artery blood supply (left anterior descending)
- may be a sign of a large anteroseptal myocardial infarct
RBBB + Left posterior fascicular block
- is less common due to a dual blood supply (right and left circumflex coronary arteries)
- Even when changes in the ECG are typical, the diagnosis should be considered only if there is no clinical evidence of right ventricle hypertrophy (RVH)
ECG findings
RBBB + Left anterior hemiblock – RBBB pattern with left axis deviation
- the frontal plane axis of the complex should be between −45 and −120 degrees
RBBB + Left posterior hemiblock – RBBB pattern with right axis deviation
- the frontal plane axis of the complex should be ≥+90 degrees
Right bundle branch block (RBBB)
- QRS duration > 120ms
- RsR’ pattern in leads V1 to V2 – M shaped, “rabbit-ear” pattern
- Deep, broad S wave in leads I, aVL and V5 to V6.
- ST segment depression and/or T wave inversion in leads V1 – V3 - altered sequence of repolarization
Left axis deviation
- QRS is POSITIVE (dominant R wave) in Lead I
- QRS is NEGATIVE (dominant S wave) in leads II, III and aVF

Right axis deviation
- QRS is POSITIVE (dominant R wave) in Lead II, Lead III and aVF
- QRS is NEGATIVE (dominant S wave) in Lead I

ECG 1 Bifascicular block (Right bundle branch block with Left posterior fascicular block)
- QRS duration 140 ms
- RsR’ / M shaped pattern in leads V1 and V2
- slurred wide S waves in leads I, aVL, V5, V6
- ST segment depression in V1, V2
- right axis deviation + 140° - left posterior fascicular block

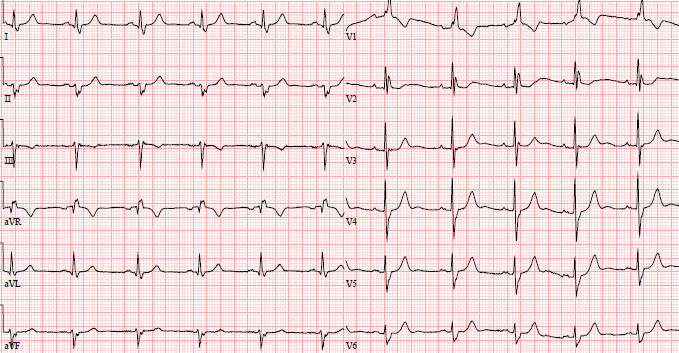
ECG 2 Bifascicular block (Right bundle branch block with Left anterior fascicular block)
- QRS duration 128 ms
- RsR’ / M shaped pattern in leads V1 and V2
- slurred wide S waves in leads I, aVL, V5, V6
Management
- The mortality may be as high as 15% in 2 years, with a 9% risk of sudden death
- Treatment should be considered only if symptoms are present due to progression of AV block (to second-degree or higher AVB)

Olshansky, B. (2017). Bifascicular block management [Graph]. In Arrhythmia Essentials (2nd ed., p. 79).
References
- Brian Olshansky, Mina K. Chung, Steven M. Pogwizd, Nora Goldschlager, Chapter 2 - Bradyarrhythmias—Conduction System Abnormalities, Editor(s): Brian Olshansky, Mina K. Chung, Steven M. Pogwizd, Nora Goldschlager, Arrhythmia Essentials (Second Edition), Elsevier, 2017, Pages 28-86, ISBN 9780323399685, https://doi.org/10.1016/B978-0-323-39968-5.00002-0.
- CAMM, A. J., LÜSCHER, T. F., & SERRUYS, P. W. (2009). The ESC textbook of cardiovascular medicine. Oxford, Oxford University Press
- STRAUSS, David G., et al. Marriott's Practical Electrocardiography. Wolters Kluwer, 2021

Introduction
- Bifascicular block is a combination of a right bundle branch block (RBBB) and a block of one of the left bundle branch fascicles – left anterior fascicular block (LAFB) or left posterior fascicular hemiblock (LPFB)
- This means that 2 of the 3 main conducting pathways through the ventricles are blocked
- Bifascicular block occurs in approx. 1% to 2% of the adult population
Causes
- Bifascicular block is often associated with structural heart disease and may be associated with progression to high-grade block or complete heart block
- The rate of progression to complete AV block is 1% to 4% per year
- In patients with syncope the rate goes up to 17% and is also associated with the presence of malignant ventricular arrhythmias
- Block in either the LAF or LPF of the LBB produces axis deviation - the overall direction of the QRS complex is shifted toward the site of the block
RBBB + Left anterior fascicular block
- more common than RBBB + LPH
- RBB and LAF have a single coronary artery blood supply (left anterior descending)
- may be a sign of a large anteroseptal myocardial infarct
RBBB + Left posterior fascicular block
- is less common due to a dual blood supply (right and left circumflex coronary arteries)
- Even when changes in the ECG are typical, the diagnosis should be considered only if there is no clinical evidence of right ventricle hypertrophy (RVH)
ECG findings
RBBB + Left anterior hemiblock – RBBB pattern with left axis deviation
- the frontal plane axis of the complex should be between −45 and −120 degrees
RBBB + Left posterior hemiblock – RBBB pattern with right axis deviation
- the frontal plane axis of the complex should be ≥+90 degrees
Right bundle branch block (RBBB)
- QRS duration > 120ms
- RsR’ pattern in leads V1 to V2 – M shaped, “rabbit-ear” pattern
- Deep, broad S wave in leads I, aVL and V5 to V6.
- ST segment depression and/or T wave inversion in leads V1 – V3 - altered sequence of repolarization
Left axis deviation
- QRS is POSITIVE (dominant R wave) in Lead I
- QRS is NEGATIVE (dominant S wave) in leads II, III and aVF
Right axis deviation
- QRS is POSITIVE (dominant R wave) in Lead II, Lead III and aVF
- QRS is NEGATIVE (dominant S wave) in Lead I
ECG 1 Bifascicular block (Right bundle branch block with Left posterior fascicular block)
- QRS duration 140 ms
- RsR’ / M shaped pattern in leads V1 and V2
- slurred wide S waves in leads I, aVL, V5, V6
- ST segment depression in V1, V2
- right axis deviation + 140° - left posterior fascicular block
ECG 2 Bifascicular block (Right bundle branch block with Left anterior fascicular block)
- QRS duration 128 ms
- RsR’ / M shaped pattern in leads V1 and V2
- slurred wide S waves in leads I, aVL, V5, V6
Management
- The mortality may be as high as 15% in 2 years, with a 9% risk of sudden death
- Treatment should be considered only if symptoms are present due to progression of AV block (to second-degree or higher AVB)
Olshansky, B. (2017). Bifascicular block management [Graph]. In Arrhythmia Essentials (2nd ed., p. 79).
References
- Brian Olshansky, Mina K. Chung, Steven M. Pogwizd, Nora Goldschlager, Chapter 2 - Bradyarrhythmias—Conduction System Abnormalities, Editor(s): Brian Olshansky, Mina K. Chung, Steven M. Pogwizd, Nora Goldschlager, Arrhythmia Essentials (Second Edition), Elsevier, 2017, Pages 28-86, ISBN 9780323399685, https://doi.org/10.1016/B978-0-323-39968-5.00002-0.
- CAMM, A. J., LÜSCHER, T. F., & SERRUYS, P. W. (2009). The ESC textbook of cardiovascular medicine. Oxford, Oxford University Press
- STRAUSS, David G., et al. Marriott's Practical Electrocardiography. Wolters Kluwer, 2021




