
Introduction
- AVRT is a supraventricular tachycardia that utilizes an accessory pathway between the atria and ventricles resulting in a circus movement
- It is frequently, but not exclusively, associated with preexcitation syndrome (ie, the Wolff-Parkinson-White syndrome)
- The circuit involved in this reentrant arrhythmia includes the accessory bypass tract, AV node, and His Purkinje system, as well as the atria and ventricles
- There is always 1:1 conduction of the impulse between the atria and ventricles since both structures, along with the AV node and accessory pathway, are a necessary part of the circuit
- AVRT is often triggered by premature atrial beats or premature ventricular beats – retrograde activation of atria
Classification and ECG findings
Based on direction of reentry circuit AVRT is divided into 2 groups:
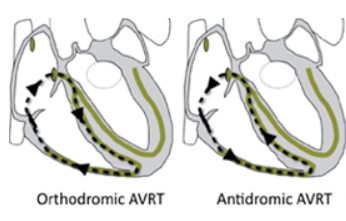
Orthodromic AVRT
- >90% of AVRT
- re-entrant impulse goes from the atria to the ventricles through the AV node (normal ventricular activation) and then retrogradely activates atria through accessory pathway
ECG:
- narrow complex tachycardia
- ventricular rate 150-250 bpm
- inverted P wave following a QRS complex - retrograde activation of the atrium
- short RP interval that is usually less than half of RR interval (< ½ RR)
Antidromic AVRT
- <10% of AVRT
- Ventricles are activated through an accessory pathway - atria are retrogradely activated over the AV node (or over another accessory pathway - some patients might have multiple accessory pathways)
ECG:
- wide QRS complex tachycardia
- ventricular rate 150-250 bpm
- Inverted P waves are often hidden in ST-T segment and therefore the RP interval is usually difficult to assess
Picture 1 Differentiation between orthodromic and antidromic AVRT
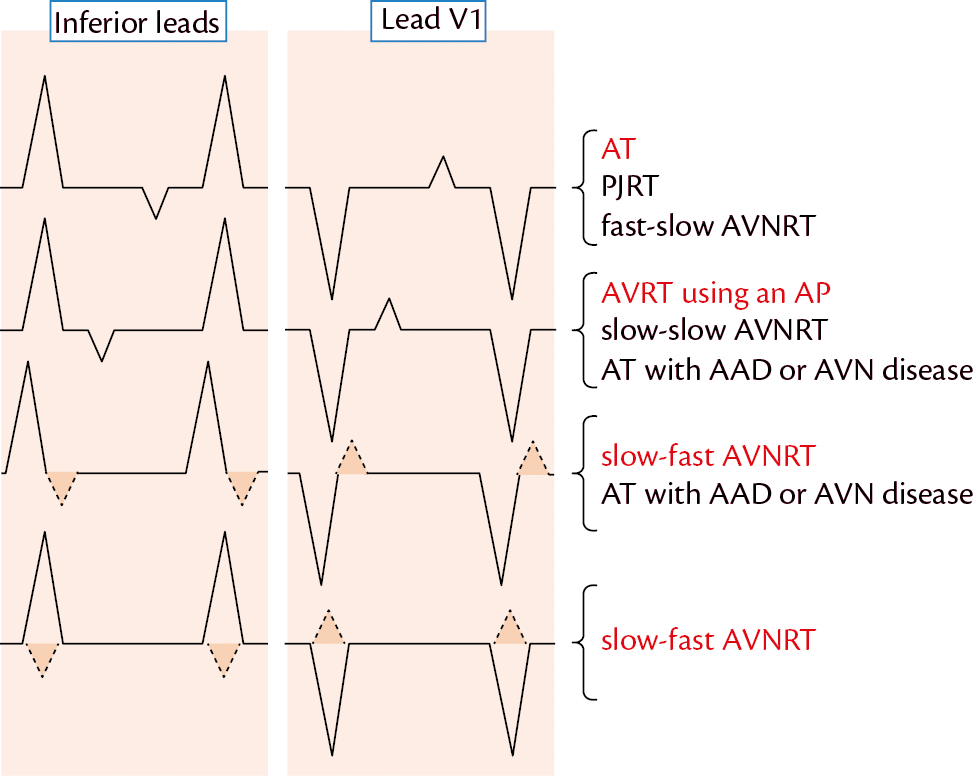
Picture 2 Differential diagnosis of supraventricular tachycardia based on the relationship of P waves and QRS complexes
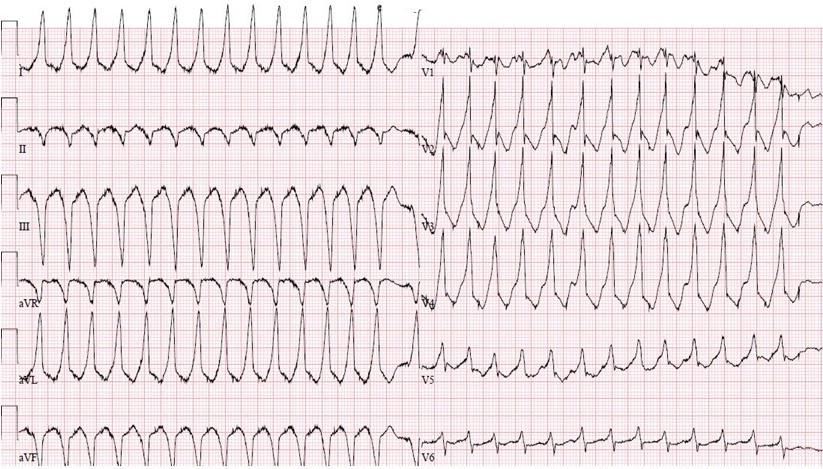
ECG 1A Antidromic atrioventricular reentrant tachycardia (AVRT)
- Regular, broad complex tachycardia, ventricular rate at 165 bpm
- retrograde P waves following QRS complexes best seen in lead V2
- left posterolateral accessory pathway origin
ECG 1B Intermittent preexcitation pattern in the same patient as above mentioned with AVRT
- this is an ECG of a patient with previous AVRT terminated by synchronized cardioversion
- narrow sinus complexes are followed by wide QRS complexes with delta waves and ST-T segment abnormalities

ECG no. 2 Wolff-Parkinson-White syndrome with orthodromic AVRT
- regular narrow complex tachycardia, ventricular rate 150 bpm
- inverted P waves following QRS complexes – short RP interval > AVNRT


Management
Acute therapy
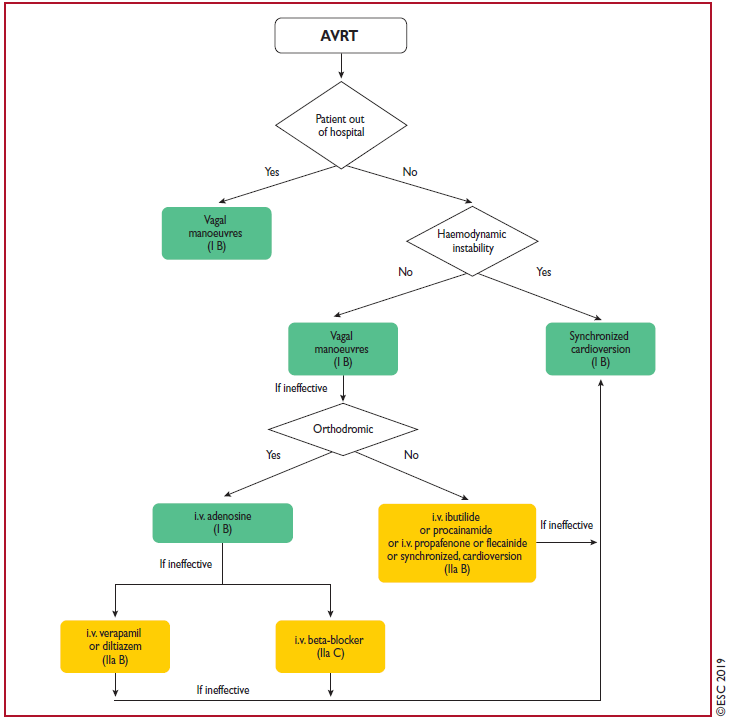
- Hemodynamically unstable patient – urgent synchronized cardioversion
- Hemodynamically stable patient
Vagal manoeuvres
- Carotid sinus massage - after auscultation of both carotid arteries (exclude significant stenosis) - pressure is applied to one carotid sinus for 5 to 10 seconds. Steady pressure is recommended because it may be more reproducible. If the expected response is not obtained, the procedure is repeated on the other side after a one- to two-minute delay.
- Valsalva manoeuvres – patient is instructed to exhale forcefully against a closed glottis (against closed mouth and compressed nose) for 10 – 15s and then release.
- Modified Valsalva manoeuvre – patient does classical Valsalva manoeuvre followed by 15 seconds of passive leg raise at 45 degree angle – this may be more successful in restoring sinus rhythm.
If vagal manoeuvres are ineffective:
- For orthodromic AVRT:
Adenosine
- use with caution! – potential induction of atrial fibrillation with fast ventricular conduction or ventricular fibrillation
- electrical cardioversion should always be available when administering adenosine
- 6 mg i.v. as a rapid bolus with saline flush
- second dose – 12 mg i.v., safe within 1 min of the last dose
- maximum dose = 18 mg
If Adenosine is ineffective > pharmacological therapy directed at AV node:
Beta blockers - i.v. esmolol, i. v. metoprolol
Calcium channel blockers (verapamil/diltiazem i.v.)
If this ineffective > Synchronized cardioversion
- For antidromic AVRT:
If vagal manoeuvres are ineffective:
Pharmacological therapy directed at fast-conducting AP (accessory pathway):
- i.v. ibutilide or procainamide
- i.v. propafenone or flecainide
Synchronized cardioversion
Chronic therapy
- The treatment of choice for patients with symptomatic and recurrent AVRT is catheter ablation of accessory pathway
- Propafenone or flecainide may be considered in patients with AVRT and without ischaemic or structural heart disease, if ablation is not desirable or feasible
Picture 3 Treatment of AVRT as per ESC guidelines
References
- CAMM, A. J., LÜSCHER, T. F., & SERRUYS, P. W. (2009). The ESC textbook of cardiovascular medicine. Oxford, Oxford University Press
- Brugada J, Katritsis DG, Arbelo E, Arribas F, Bax JJ, Blomström-Lundqvist C, Calkins H, Corrado D, Deftereos SG, Diller GP, Gomez-Doblas JJ, Gorenek B, Grace A, Ho SY, Kaski JC, Kuck KH, Lambiase PD, Sacher F, Sarquella-Brugada G, Suwalski P, Zaza A; ESC Scientific Document Group. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J. 2020 Feb 1;41(5):655-720. doi: 10.1093/eurheartj/ehz467. PMID: 31504425.
- Luigi Di Biase, MD, PhD, FHRS, Edward P Walsh, MD (2019). Atrioventricular reentrant tachycardia (AVRT) associated with an accessory pathway In I. Susan B Yeon, MD, JD, FACC (Ed.), UpToDate. Retrieved February 3, 2021 from https://www-uptodate-com.ezproxy.is.cuni.cz/contents/atrioventricular-reentrant-tachycardia-avrt-associated-with-an-accessory-pathway?search=avrt&source=search_result&selectedTitle=1~84&usage_type=default&display_rank=1
- Oxford Medicine Online. Oxford Medicine Online Differential diagnosis of supraventricular tachycardias : ESC CardioMed
Picture no. 1 - https://thoracickey.com/atrioventricular-reciprocating-tachycardia/
Picture no. 2 - Oxford Medicine Online. Oxford Medicine Online Differential diagnosis of supraventricular tachycardias : ESC CardioMed
Picture no. 3 Acute therapy of atrioventricular reentrant tachycardia. (2019). [Graph]. Accessible at: https://academic.oup.com/eurheartj/article/41/5/655/5556821

Introduction
- AVRT is a supraventricular tachycardia that utilizes an accessory pathway between the atria and ventricles resulting in a circus movement
- It is frequently, but not exclusively, associated with preexcitation syndrome (ie, the Wolff-Parkinson-White syndrome)
- The circuit involved in this reentrant arrhythmia includes the accessory bypass tract, AV node, and His Purkinje system, as well as the atria and ventricles
- There is always 1:1 conduction of the impulse between the atria and ventricles since both structures, along with the AV node and accessory pathway, are a necessary part of the circuit
- AVRT is often triggered by premature atrial beats or premature ventricular beats – retrograde activation of atria
Classification and ECG findings
Based on direction of reentry circuit AVRT is divided into 2 groups:
Orthodromic AVRT
- >90% of AVRT
- re-entrant impulse goes from the atria to the ventricles through the AV node (normal ventricular activation) and then retrogradely activates atria through accessory pathway
ECG:
- narrow complex tachycardia
- ventricular rate 150-250 bpm
- inverted P wave following a QRS complex - retrograde activation of the atrium
- short RP interval that is usually less than half of RR interval (< ½ RR)
Antidromic AVRT
- <10% of AVRT
- Ventricles are activated through an accessory pathway - atria are retrogradely activated over the AV node (or over another accessory pathway - some patients might have multiple accessory pathways)
ECG:
- wide QRS complex tachycardia
- ventricular rate 150-250 bpm
- Inverted P waves are often hidden in ST-T segment and therefore the RP interval is usually difficult to assess
Picture 1 Differentiation between orthodromic and antidromic AVRT
Picture 2 Differential diagnosis of supraventricular tachycardia based on the relationship of P waves and QRS complexes
ECG 1A Antidromic atrioventricular reentrant tachycardia (AVRT)
- Regular, broad complex tachycardia, ventricular rate at 165 bpm
- retrograde P waves following QRS complexes best seen in lead V2
- left posterolateral accessory pathway origin
ECG 1B Intermittent preexcitation pattern in the same patient as above mentioned with AVRT
- this is an ECG of a patient with previous AVRT terminated by synchronized cardioversion
- narrow sinus complexes are followed by wide QRS complexes with delta waves and ST-T segment abnormalities
ECG no. 2 Wolff-Parkinson-White syndrome with orthodromic AVRT
- regular narrow complex tachycardia, ventricular rate 150 bpm
- inverted P waves following QRS complexes – short RP interval > AVNRT
Management
Acute therapy
- Hemodynamically unstable patient – urgent synchronized cardioversion
- Hemodynamically stable patient
Vagal manoeuvres
- Carotid sinus massage - after auscultation of both carotid arteries (exclude significant stenosis) - pressure is applied to one carotid sinus for 5 to 10 seconds. Steady pressure is recommended because it may be more reproducible. If the expected response is not obtained, the procedure is repeated on the other side after a one- to two-minute delay.
- Valsalva manoeuvres – patient is instructed to exhale forcefully against a closed glottis (against closed mouth and compressed nose) for 10 – 15s and then release.
- Modified Valsalva manoeuvre – patient does classical Valsalva manoeuvre followed by 15 seconds of passive leg raise at 45 degree angle – this may be more successful in restoring sinus rhythm.
If vagal manoeuvres are ineffective:
- For orthodromic AVRT:
Adenosine
- use with caution! – potential induction of atrial fibrillation with fast ventricular conduction or ventricular fibrillation
- electrical cardioversion should always be available when administering adenosine
- 6 mg i.v. as a rapid bolus with saline flush
- second dose – 12 mg i.v., safe within 1 min of the last dose
- maximum dose = 18 mg
If Adenosine is ineffective > pharmacological therapy directed at AV node:
Beta blockers - i.v. esmolol, i. v. metoprolol
Calcium channel blockers (verapamil/diltiazem i.v.)
If this ineffective > Synchronized cardioversion
- For antidromic AVRT:
If vagal manoeuvres are ineffective:
Pharmacological therapy directed at fast-conducting AP (accessory pathway):
- i.v. ibutilide or procainamide
- i.v. propafenone or flecainide
Synchronized cardioversion
Chronic therapy
- The treatment of choice for patients with symptomatic and recurrent AVRT is catheter ablation of accessory pathway
- Propafenone or flecainide may be considered in patients with AVRT and without ischaemic or structural heart disease, if ablation is not desirable or feasible
Picture 3 Treatment of AVRT as per ESC guidelines
References
- CAMM, A. J., LÜSCHER, T. F., & SERRUYS, P. W. (2009). The ESC textbook of cardiovascular medicine. Oxford, Oxford University Press
- Brugada J, Katritsis DG, Arbelo E, Arribas F, Bax JJ, Blomström-Lundqvist C, Calkins H, Corrado D, Deftereos SG, Diller GP, Gomez-Doblas JJ, Gorenek B, Grace A, Ho SY, Kaski JC, Kuck KH, Lambiase PD, Sacher F, Sarquella-Brugada G, Suwalski P, Zaza A; ESC Scientific Document Group. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J. 2020 Feb 1;41(5):655-720. doi: 10.1093/eurheartj/ehz467. PMID: 31504425.
- Luigi Di Biase, MD, PhD, FHRS, Edward P Walsh, MD (2019). Atrioventricular reentrant tachycardia (AVRT) associated with an accessory pathway In I. Susan B Yeon, MD, JD, FACC (Ed.), UpToDate. Retrieved February 3, 2021 from https://www-uptodate-com.ezproxy.is.cuni.cz/contents/atrioventricular-reentrant-tachycardia-avrt-associated-with-an-accessory-pathway?search=avrt&source=search_result&selectedTitle=1~84&usage_type=default&display_rank=1
- Oxford Medicine Online. Oxford Medicine Online Differential diagnosis of supraventricular tachycardias : ESC CardioMed
Picture no. 1 - https://thoracickey.com/atrioventricular-reciprocating-tachycardia/
Picture no. 2 - Oxford Medicine Online. Oxford Medicine Online Differential diagnosis of supraventricular tachycardias : ESC CardioMed
Picture no. 3 Acute therapy of atrioventricular reentrant tachycardia. (2019). [Graph]. Accessible at: https://academic.oup.com/eurheartj/article/41/5/655/5556821




